


Addison’s In Cats
Scratching out information in scarcity


As a 4th year in vet school, I dated a man with hypoadrenocorticism. One day, as I was studying for boards, I found him seizing with a HR of 30, a respiratory rate of 5, nearly dead. When the ambulance got to my house, the medics kept asking me what he had taken… it wasn’t what he took but rather what he was not taking. Profound bradycardia, BP tanked, and his BG was in the toilet. I kept telling them that his potassium was too high, and that he needed dextrose, steroids, and shock dose NaCl.
I had to miss that afternoon’s ICU shift at the vet school, but I got an education. The profound effects of the Addisonian crisis made an impression on me. On my next ICU shift, my clinical professor and I discussed my boyfriend’s case. They, not so jokingly, suggested I keep a bottle of Solu-delta-cortef and a bag of NaCl at home.
Caveat Imitator
Addison’s is one of medicine’s “the great imitators” because sometimes the signs can be super vague and the changes subtle. But sometimes, the signs hit you over the head with a sledgehammer. Even when looking at a signalment that does not jive with the differential diagnosis. To preface this, Addison’s in cats is rare. And Addison’s in a cat under 1 year of age is SUUUUUPPPPER rare. That being said, it may be underdiagnosed- the assumption being a diagnosis of renal failure rather than ADrenal failure.

Enter my kitten patient, “D.”
At 15 weeks old, he had failure to thrive, unlike his littermate who was double his weight. The labs were classic: mild azotemia with a low Na:K, dilute urine. I told the owners that it was a moonshot but that I wanted to do a resting cortisol and probably an ACTH stim test. In the end, I ran a stim in-house and sent parallel samples to Idexx to confirm because I still didn’t really believe the results. It looked like my 15 week old kitten had Addison’s.
Research mode begins
When I find myself faced with a disease process that I am not familiar with or want to update my understanding, I create a document where I dump citations and bullet points from each. From this document, I use ChatGPT to create algorithms.
This kind of research has its limitations.
It is biased.
I choose what sources to use.
I choose what information from each source to put in the database.
2. It requires education.
Understanding how to choose and weigh sources is important
An advanced to expert level of understanding is needed to ensure that the output is correct.
Choosing what information to include in your bullet points will skew results and you need to know what is important.
Knowing how to formulate the prompt to weigh the order of testing and preference for treatments is required.
3. Being a fast reader is vital.
Reading through each source takes time
Back to my kitten case.

While I had my citations and information from the point of the original diagnosis, I didn’t create an algorithm until today. For months, “D” rocked along, improving with the regular DOCP injections and prednisolone syrup. Until, one day, even though it was around day 28 and his Na:K had dropped to an appropriately low level, his normal dose of DOCP shot his Na:K ratio through the roof within 2 hours.
Cue scrambling to consult with Dechra on Zycortal use in cats, supportive care, IM consult, oral potassium supplementation, and increased prednisolone.
I dropped the dose of Zycortal at the next monthly electrolyte check by 25%. He was fine for 4 days, then had a series of seizures: his sodium and potassium both jumped up. “D” was treated for presumed electrolyte imbalance due to the DOCP administration and started Keppra briefly. We pulled him out of that nose dive. And now I was faced with what to do on his next go around.
It was time to create an algorithm for Addison’s treatment in cats using the previous data information, rolling in the suggestion of dropping the DOCP dose given by the technical veterinarian at Dechra as well as some more pointed research on moving to Fludrocortisone and Prednisolone dosing. With my new information document uploaded, I requested ChatGPT to generate an algorithm for treatment in a cat diagnosed with Addison’s.
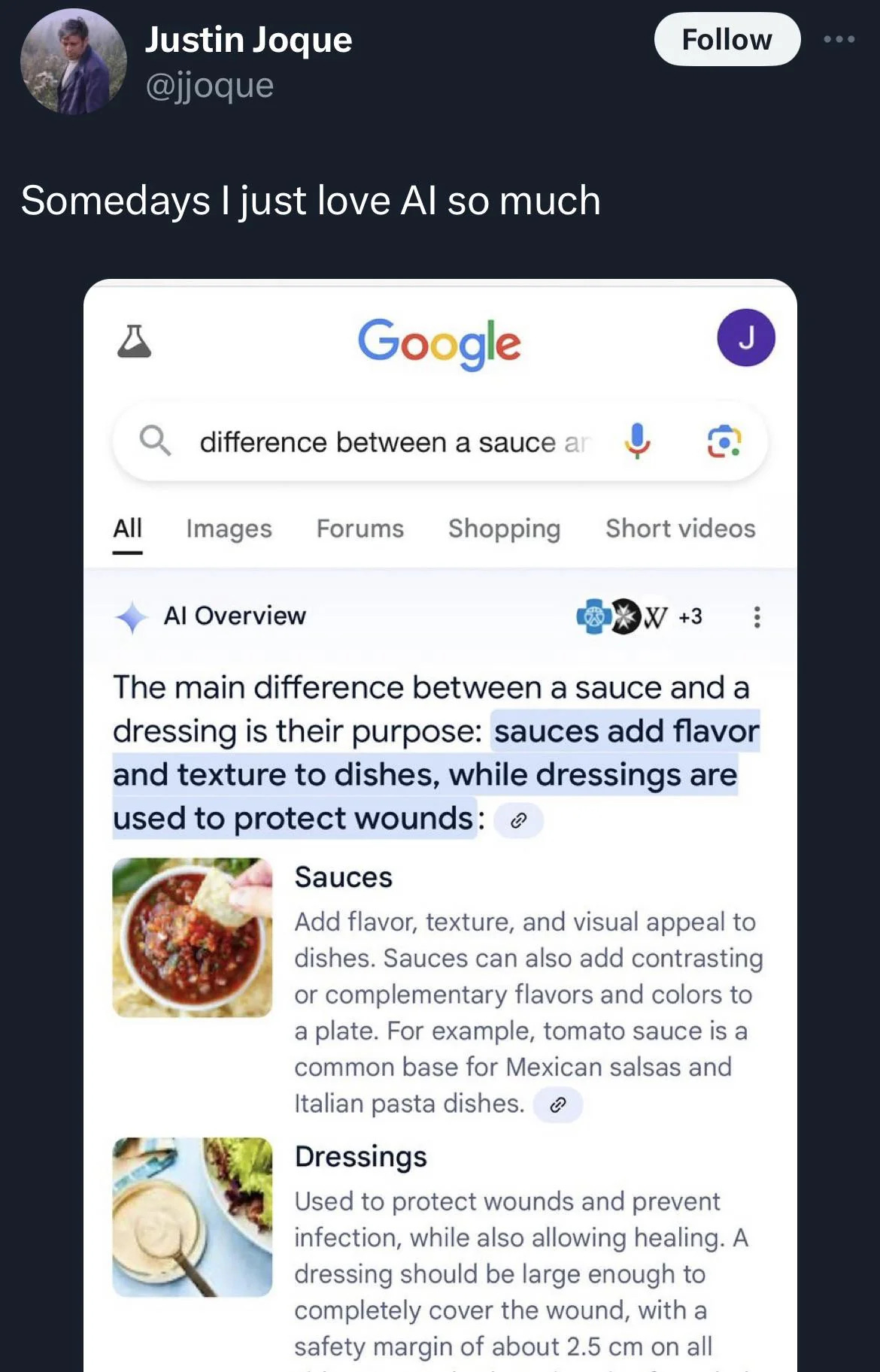
When you are giving AI the information to pull from, you virtually eliminate the chance for hallucination. Ask AI to create a complicated document whole cloth is asking for a treatise on sauces and dressings and getting a response that includes bandaging material.
Initial prompt:
“Create an algorithm for managing a young cat diagnosed with Addison’s disease. Include both options for using DOCP/prednisolone and Fludrocortisone/Pred regimens, with DOCP/Pred as the first choice. Include a schedule for rechecking labs and indications for a need for changes in dosing. Include the information that after a crisis potentiated by a Zycortal inj, Dechra advised that the subsequent feline dose should be decreased by 25%.”
The first output was ok, but didn’t include any specifics on titrating the prednisolone dosing amount and frequency.
Follow-up Prompt:
“Specifically, how often should the pred be given in conjunction with the florinef?”
Output:
When using Florinef (fludrocortisone) for a cat with Addison’s disease, prednisolone is still typically needed, but at a lower dose and potentially less frequently, since Florinef has both mineralocorticoid and glucocorticoid activity.
Florinef + Prednisolone Dosing Strategy
Florinef
Dose: 0.01–0.02 mg/kg every 12 hours (BID).
Adjust based on Na/K levels and clinical signs.
Prednisolone
Start low: 0.05–0.1 mg/kg once daily.
Some cats may not need daily dosing — alternate-day or “every 2–3 days” can be considered once stable.
If signs of glucocorticoid deficiency occur (lethargy, anorexia, vomiting, weight loss), increase dose or frequency temporarily.
Stress situations (travel, illness, vet visits): Double the pred dose for 1–2 days.
More Fiddling Around
I asked for an updated algorithm that included prednisolone titration info, but the first version missed an important detail—it didn’t list “every-three-days” as a valid low-end dosing option. Once I fixed that and tweaked a few other small things, I ended up with something usable.
What this system lets me do is basically what we do all the time as vets: take in the info, figure out what matters for the case or condition, and build a plan from there. The difference is, instead of mentally juggling all the dosing schedules and follow-up steps, you get a tailored plan built from the same knowledge you'd normally use—just more organized and ready to go.
It is a banger reference to have handy and one that you can easily update every time you come across new information. The act of creating a pool of citations/data dumps results in improved apprehension of the information. Reading through the output and making adjustments based on checking your sources further cements your handle on it.
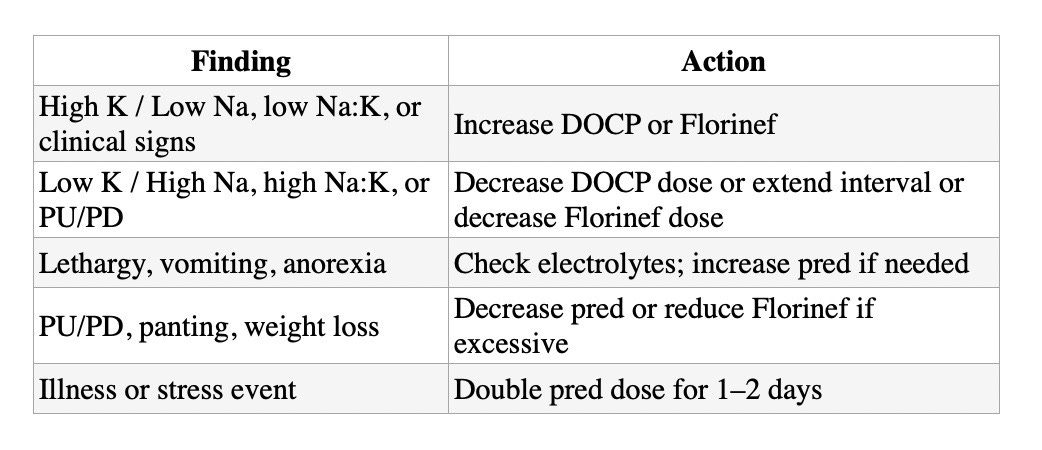
Final Output (specific to a cat with Addison’s disease)
Here is the good stuff. Now have something that I can use when faced with the multitude of feline Addisonian patients sure to be coming down the pike. Note, I did not include initial diagnostics nor dig into emergency stabilization.
Feline Addison’s Disease Management Algorithm
1. Initial Stabilization
If the cat presents in an Addisonian crisis:
IV fluids: 0.9% NaCl.
IV glucocorticoid: Dexamethasone SP (compatible with ACTH testing).
Correct electrolytes, glucose, and stabilize vitals.
Once stable, begin maintenance therapy.
2. Maintenance Therapy Options
Primary Protocol: DOCP (Zycortal) + Prednisolone
DOCP (Zycortal)
Initial dose: 2.2 mg/kg SC every 28 days.
Post-crisis: If crisis followed a dose, reduce next dose by 25% (Dechra guidance).
Example: 2.2 mg/kg → reduce to ~1.65 mg/kg.
Adjust dose or frequency based on clinical signs and serum electrolytes.
Prednisolone
Start: 0.5–1.0 mg/kg/day PO.
Taper over weeks to:
Maintenance: 0.1–0.3 mg/kg/day.
Stress dosing: Double the dose for 1–2 days during illness or high-stress events.
Secondary Protocol: Florinef (Fludrocortisone) + Prednisolone
Florinef
Start at 0.01–0.02 mg/kg PO every 12 hours (BID).
Adjust every 1–2 weeks based on serum Na/K and clinical response.
Be aware that cats may develop a need for increasing doses over time.
Prednisolone
Start: 0.05–0.1 mg/kg once daily PO.
Taper to the lowest effective dose and frequency:
Maintenance options: daily, every other day, every 3 days, or even twice weekly, depending on the cat’s clinical stability.
Stress dosing: Double for 1–2 days during illness, travel, or procedures.
3. Monitoring and Rechecks
Electrolytes (Na/K)
DOCP protocol:
Day 10–14 after injection (peak effect).
Day 25–28 (trough, pre-next injection).
Florinef protocol:
Recheck Na/K every 1–2 weeks initially.
Once stable: every 1–3 months.
Routine Rechecks
First 3 months: monthly monitoring.
Stable patients: recheck every 2–3 months.
Annual workup: CBC, chemistry, urinalysis.
4. Dose Adjustments: When & Why
Beyond the algorithm
From the same information set and output, you can request a staff training handout, a client handout, and social media posts. You can even go further and combine a patient history summary with an algorithm and create a personalized plan.